

Objective
To assess in-class transition (iCT) from intravenous bortezomib-based induction to all-oral ixazomib-based treatment improving proteasome inhibitor-based continuous therapy with efficiency, safety and convenience in clinical practice.
Methods
In this real-world retrospective study from Chinese seven hospitals during Oct, 2017-Jul, 2020, we analysed newly diagnosed multiple myeloma (NDMM) patients without transplantation, who achieved at least partial response of bortezomib-based introduction, and then received ixazomib-based regimen for 2 years or until progression/intolerant toxicity. Primary endpoint: progression-free survival (PFS). Key endpoints included response rate, therapy duration and adverse event (AE).
Results
96 patients were enrolled in this study (median age 61 years; 25% ≥ 65 years; 7% ≥ 75 years; 61% male; ISS stage I/II/III 10%/35%/55%; IgG/IgA/IgD/IgE/light chain /double clonal /non-secretory 50%/18%/2%/1%/26%/1%/2%). R-ISS stage was estimated in 85 patients (stage I/II/III 6%/78%/16%). 35% high risk(HR) (27/78) and 65% standard risk (SR)(51/78) were tested by metaphase fluorescence in situ hybridization (M-FISH) according to Mayo clinic risk stratification.
96 patients received median 5 cycles (2-12) of bortezomib-based regimen including VD1/VRD1/VTD1/VCD1/PAD1/PD2D1, and median 6 cycles (1-17) of iCT regimen including ID1/IRD1/ITD1/ICD1 (30/96,43/96,10/96,13/96), three-drug ixazomib-based regimens account for the majority (66/96). Median duration of total PI therapy was 11.3 months and of ixazomib-based regimen was 5.3 months.
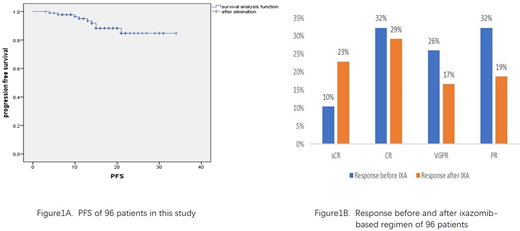
With 13 months median follow-up, 18-month progression free survival (PFS) rate was 87% (95% confidence interval,78-95) from the start of bortezomib-based induction and 82% (95% confidence interval,70-94) from the start of ixazomib-based treatment(Figure 1A), 79% patients remain on therapy at data cutoff. After bortezomib-based induction, overall response(ORR) rate was 100% (strict complete response [sCR], 10/96, 10%; complete response [CR], 31/96, 32%; very good partial response [VGPR], 24/96, 26%; partial response [PR], 31/96, 32%) and 88% (sCR 22/96, 23%; CR, 28/96, 29%; VGPR, 16/96, 17%; PR, 18/96, 19%) at data cutoff. There were 3 PR improved to VGPR, 4 VGPR improved to CR, 1 PR, 4 VGPR and 5 CR improved to sCR (Figure 1B). ORR of HR patients were 100% and 85%(23/27), 1 PR improved to VGPR, 1PR improved to CR, 4CR improved to sCR; ORR of SR patients were 100% and 85% (45/51), 2PR improved to VGPR, 5VGPR improved to CR, 4VGPR and 3CR improved to sCR, before and after ixazomib-based regimen, respectively.
Among 66 patients who transited to IRD1/ITD1/ICD1 regimen, medium duration of total PI therapy was 11.0 months and of ixazomib-based regimen was 5.4 months, 77% patients remain on therapy. ORR rate was 100% (sCR, 7/66, 11%; CR, 16/66, 24 %; VGPR, 16/66, 24%; PR, 27/66, 41%) and 91% (sCR 15/66, 23%; CR, 18/66, 27%; VGPR, 9/66, 14%; PR, 18/66, 27%) at data cutoff, 3 PR improved to VGPR, 4PR and 6 VGPR improved to CR, 4 VGPR and 3 CR improved to sCR. ORR of HR (23/52) patients were 100% and 96%, ORR of SR patients (29/52)were 100% and 86% before and after ixazomib-based regimen, respectively.
The ixazomib-safety profile was consistent with previous clinical trial data. In our study, 59% (57/96) of patients had any grade adverse events AE. In which, the most frequent grade <=2 AEs were peripheral neuropathy(PN) (31%, 31/96, PN of 23 patients began after bortezomib-based induction), nausea and vomiting (33%), diarrhea (5%), constipation (4%), incomplete intestinal obstruction (3%), fatigue (2%), edema (1%), abdominal distension (1%) , anorexia (1%), rash(1%) , weakness of lower limbs (1%). The most frequent grade 3/4 AEs were agranulocytosis (2%) , rash (2%), PN (2%, occurred after bortezomib-based induction). Treatment discontinued of ixazomib-based regimen are PN (6/96), incomplete intestinal obstruction (1/96), agranulocytosis (1/96), rash (2/96).
Conclusion
In real-world China MM population, NDMM patients are sensitive to PI-based continuous therapy with satisfied response rate; iCT can permit prolonged PI-based therapy with promising efficacy and tolerated adverse events.
Note:
VD1, VRD1, VTD1, VCD1, PAD1, PD2D1, IRD1, ITD1, ICD1 :
I: ixazomib, R: lenalidomide, T: thalidomide, C: cyclophosphamide,
V: bortezomib, D1: dexamethasone P: bortezomib, A: adriamycin
D2: liposome doxorubicin
No relevant conflicts of interest to declare.

